GENERAL MEDICINE E-LOG
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
CHIEF COMPLAINT:
A 63 yr old male came to the opd with the chief complaints of
- Sleep disturbances
- Low mood since 1 year
Patient was apparently asymptomatic 2 years back after which he developed a lesion over right leg Just above the ankle joint which was insidious in onset, gradually progressive in nature. Patient sought medical care from different health care professionals, but instead of subsiding,the lesions grew in size from initial size of a coin to present size and also got diffuse despite receiving various treatments.
Patient complaints of low mood since past 1 year due to diffuse distribution of lesions which are prominently visible and the pain itching associated with it. Patient is scared that it might be contagious, so he lives by himself in his room,stays to himself, washes his clothes, doesn’t eat food unless someone asks him to. He doesnt work like he uesd to before the onset of lesions. Before he used to wake up early in the morning do his regular activities, go for a walk in the village, talk to people, attend the functions of his fellow villagers as he is from one of the reputed families in the village. But since the onset of condition, he is scared of persecution from the villagers and doesnt go out and stays in the house since past year.
Patient complaints of sleep disturbances since past 1 year due to the fear of his condition being contagious. Before he used to sleep early in the night, have undisturbed sleep, and wake up early in the morning and do his regular activities. Lately since 1 year he cannot sleep even late at night, even then he wakes up atleast twice in the night.
Patient also gives history of suicidal indications.
Patient gives history of alcohol consumption past 35 years.Initially he used to consume 3 to units units of alcohol per week for 10 years. Then he started consuming 6-9 units per week. Currently he consumes 6-9 units per day everyday since past 2 days, since the onset of his skin condition, his last drink was a week back where he consumed 3 units. Patient mentions that since his condition started he is consuming more due to his inability to sleep, because of pain and itching.
Patient also gives history of smoking tobacco since past 35 years, it started with occasional smoking when he consumes alcohol, initially progressed to 4-5 cigarettes per day everyday since past 30 years. Craving were present, last smoke was 3 days ago, loss of control is present, c/o dry mouth.
Recently patient went to psychiatrist in suryapet 3 days ago where he was asked to abstain from smoking and drinking and was put on medication to prevent any withdrawal and was suggested to go Kamineni hospital, Narketapally for his skin condition and for supervised detoxification.
No H/O blood in stool/vomitus/urine, seizure like activity.
No H/O other substance use, suspiciousness, hearing of voices, overvalued ideas, grandiosity, repetitive thoughts.

PAST HISTORY:
N/K/c/o - DM, HTN, Broncial asthma, TB
FAMILY HISTORY:
- Lower middle socioeconomic status
- Interpersonal relationships maintained
PERSONAL HISTORY:
- Appetite is decreased
- Having mixed diet
- Bowels regular
- Micturition normal
- Alcohol intake was present
- Has a habit of smoking
- No other habits/ addictions
Patient is conscious, coherent
Absence of pallor, icterus, clubbing, cyanosis, pedal edema, lymphadenopathy.
VITALS:
1.Temperature: 98 F
2.Pulse rate: 85 beats per min
3.Respiratory rate: 16 cycles per min
4.BP: 120/70mm Hg
5.SpO2: 98% @ Room air
6.GRBS: 172mg%
SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM:
- S1, S2 heard
- No thrills, No murmurs
RESPIRATORY SYSTEM:
- Normal vesicular breath sounds
- Position of trachea is central
- Dyspnea is absent
- No wheeze
EXAMINATION OF ABDOMEN:
- Shape- scaphoid
- No tenderness
- No palpable pass
- Normal hernial orifices
- No free fluid
- No Bruits
- Liver is not palpable
- spleen is not palpable
- Bowel sounds heard
CENTRAL NERVOUS SYSTEM:
- Patient is conscious
- Speech is normal
- No focal neurological defect
- All reflexes were present
- Absence of cerebral signs
ALCOHOL DEPENDENCE SYNDROME
TOBACCO DEPENDENCE SYNDROME
ADJUSTMENT DISOREDR DUE TO PHYSICAL ILLNESS
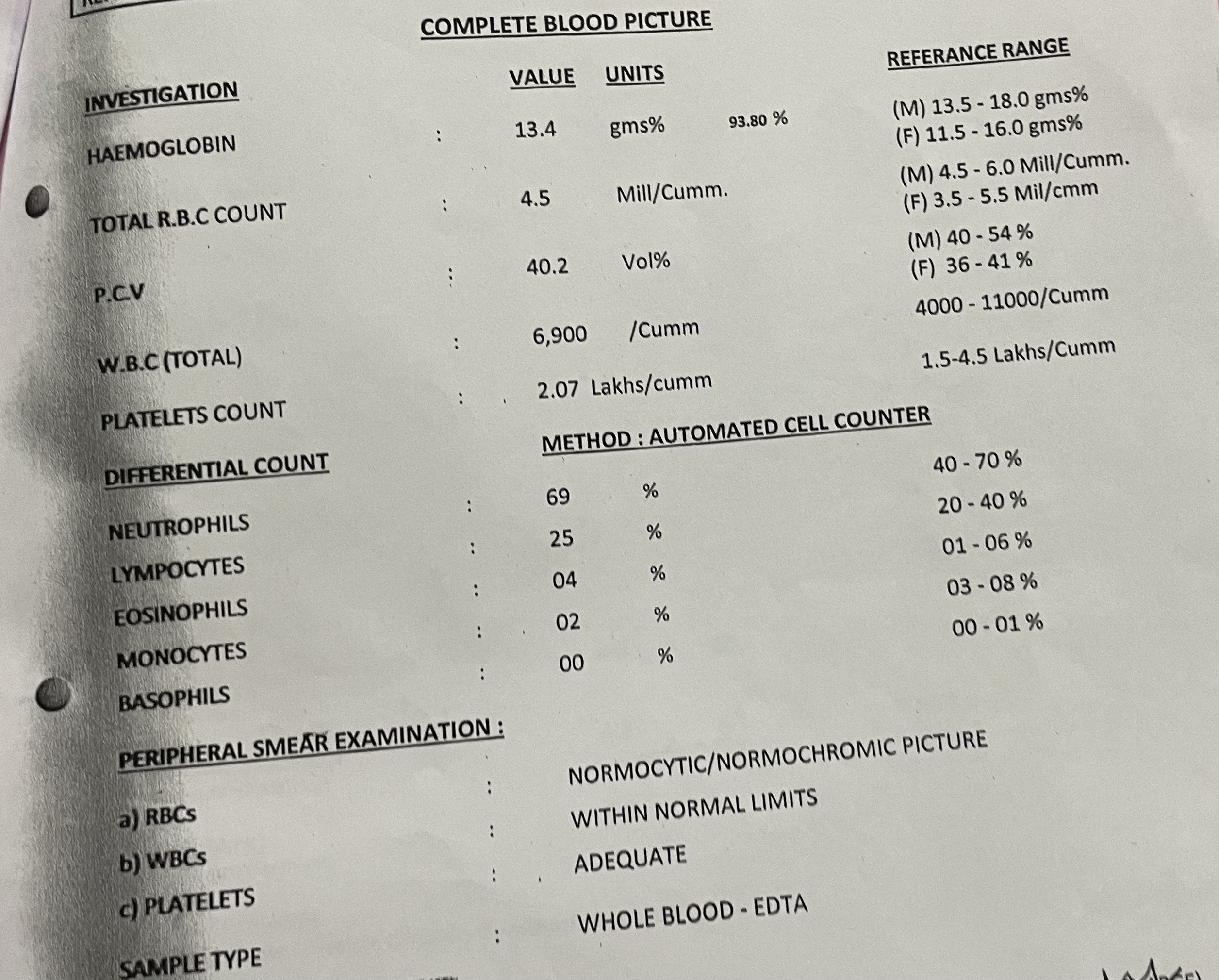
INVESTIGATIONS:
Investigations on 3/06/22:





- Tab.Lorazepam 2mg for 5 days
- Tab.Benfothiamine 100mg
- Tab.Sertraline 25mg
- Nicotex gums 2mg
- Tab.Lorazepam 2mg
- Tab.Benfothiamine 100mg
- Tab.Sertraline 25mg
- Liquid paraffin
- Tab.Atorvastatin 20mg
- Tab.Lorazepam 2mg
- Tab.Benfothiamine 100mg
- Tab.Sertraline 25mg
- Liquid Paraffin
- Tab.Atorvastatin 20mg
- Tab.Drotin P SOS
- Syp.Citralka 10ml
- Tab.Lorazepam 2mg
- Tab.Benfothiamine 100mg
- Tab.Sertraline 25mg
- Liquid Paraffin
- Tab.Atorvastatin 20mg
- Tab.Drotin P SOS
- Syp.Citralka 10ml
- Tab.Atarax 25mg
- Fudic cream l/a
- Venusia cream l/a
Comments
Post a Comment